Blood flows
Aorta is the largest artery in the cardiovascular system. The main function of the aorta is to transport oxygen-rich blood to the other arteries. The ascending aorta is emanated from the Left Ventricle and forms a curvature along the aortic arch. The descending aorta lays up to the thoracic aorta. The aorta has a higher distensibility compared to the other arteries. The elastic aortic walls allow aorta to respond to the flow and pressure variations. The aorta expands during the systole, when the heart pumps out blood into the ascending aorta passing through the heart valves to store about 50% of the left ventricle stroke volume. It contracts in diastole, when the heart is in rest mode, to eject the stored volume. The flow in the aorta is pulsatile and three dimensional. The complex geometry, pulsatility, three dimensionality and the non-stationary boundaries in each pulse are significant factors affecting the flow patterns. The existence of turbulence has not been completely proved in aorta. Disturbed flow is believed as one of the key factors for cardiovascular diseases. It is assumed that the flow becomes turbulent in large arteries such as aorta.
Arrhythmogenic Right Ventricular Cardiomyopathy/Dysplasia (ARVC/D)
The pathophysiologic processes leading to structural alterations of the right ventricle (RV) in the athlete’s heart and in patients with arrhythmogenic right ventricular cardiomyopathy/dysplasia (ARVC/D) are incompletely understood. Although disease mechanisms due to abnormal blood flow and mechanical stresses have extensively been studied for the left heart, in particular for the left ventricle (LV) and the aorta, there is a paucity of data analyzing these processes for the right heart. In particular, there is a lack of in vitro models to study the right heart except for few studies investigating the function of the right-sided valves and some forms of congenital heart disease. The complex anatomy and physiology of the right heart contribute to the difficulty to create appropriate in vitro models to study the influences of mechanical forces on disease mechanisms within these cardiac chambers. ARVC/D is a unique hereditary disease, which predominantly affects the RV. It is characterized by progressive replacement of myocardium by fibro-fatty tissue. ARVC/D is a common cause of sudden cardiac death, particularly in young adolescents and athletes. The RV has structural abnormalities such as wall thinning and aneurysm formation. The impact of abnormal blood flow and mechanical stresses on the pathogenesis of structural alterations in ARVC/D and their predilection sites has not been studied to date.
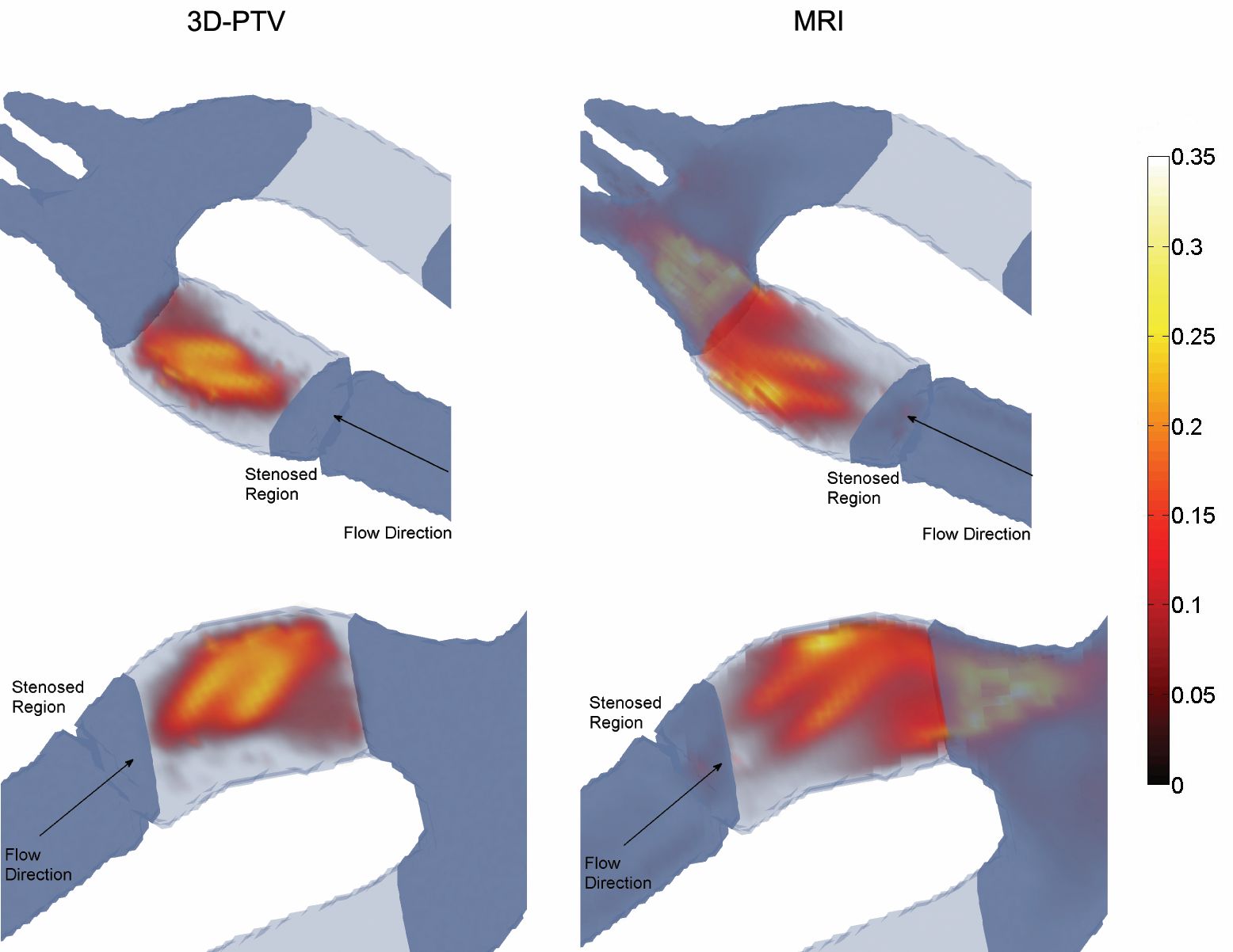
Stenotic Flows
Aortic stenosis is one of the most common heart diseases in the Western world and can lead to ventricular dysfunction, heart failure, and death. Aortic stenosis results as a consequence of calcification of aortic valve leaflets and hence leads to abnormalities in the blood flow. In diseased aortic valves, the cusps of the valve become stiffer and the movement of the cusps is limited which provokes a reduction in the effective orifice area and considerably higher blood velocities. Up to now functional assessment and risk assessment is mostly based on measurements of either blood flow velocity or pressure, which rely on several assumptions and are subject to significant uncertainty. In clinical routine, pressure gradients and effective orifice area are used as measures of aortic stenosis severity. A common method is to measure the pressure loss via a catheter. However, this method is invasive and it provides only limited information on stenosis characteristics that is often insufficient e.g. for the planning of clinical intervention. Doppler echocardiography is the standard tool to assess the severity of a stenosis. It has, however, been noted that it is affected by significant uncertainty due to technical and conceptual limitations of Doppler echo, i.e. the assumption of laminar flow with flat velocity profiles at the vena contracta, difficulties in the alignment of Doppler and blood flow intercept angle and the inability of assessing pressure recovery. Therefore, there is a need for establishing alternative non-invasive methods capable of providing more complete and accurate information on stenosis severity.